Assistant Professor, Southwestern Pennsylvania (school name TBD)
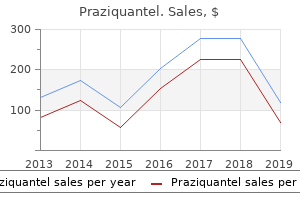
Jonsen 20 has formulated the following situations in which futility should be considered: (1) futility in process treatment 2 prostate cancer purchase praziquantel in united states online, in which a long and difficult course continues without any improvement; (2) futility in prognosis acute treatment buy praziquantel 600mg, when patients start treatment that has rarely or never proved useful in similar cases; (3) futility in result medications kidney infection generic praziquantel 600mg online, when treatment is technically successful but the resulting quality of life is undesirable symptoms crohns disease order discount praziquantel. Recognizing these junctures and communicating them to patients and families requires physician sensitivity to the philosophy and practice of palliative care. During such discussions, the physician can state that cure or control of disease is no longer possible. Each physician must use his or her experience to influence the proper choice, always supporting the patient in the final decision and never implying disappointment, anger, or abandonment. Where patient and family insist on or demand futile treatments, it is incumbent upon the physician to begin discussion of palliative care as an acceptable option. Furthermore, the possibility for hope and the new goal of maintaining quality of life through palliative care are emphasized. Patients and families should understand that their role in developing symptom management may be greater than their role in directing curative therapies. This shift in goals and participation is a significant part of the process for patients and families in dealing with the end of life. Many patients have fears and beliefs that make it difficult for them to accept palliative rather than curative care. Patients may fear that accepting death means that they will experience abandonment and isolation as both their families and medical care givers "give up" on them. They may foresee uncontrolled pain and suffering and devaluation of their personhood. Physicians should be mindful that these concerns may hinder patients from finding hope in the decision to seek palliative care, and they should openly discuss the support provided by palliative care programs. Patients may use this decision point to resolve these interpersonal issues and to seek closure. Hospice caregivers are trained to assist patients in reviewing their lives, thereby affirming self-worth. The physician receives support from that team and, in turn, can help empower patients to see their medical care and symptom management as part of a more comprehensive approach to terminal illness. The following section describes in greater detail the most common symptoms encountered at the end of life and the options available to physicians, patients, and families. Symptom Prevalence in Cancer Patients at Various Stages of Disease Several important points about symptom prevalence are not evident from Table 56. In one study of the last 48 hours of life, 22% of patients had worsening of previously controlled pain, and 30% had new pain. Readers should consult the review by Ingham and Portenoy 34 for extended discussion of symptom assessment tools. The signs and symptoms of failure to thrive are a prime example of constitutional change and occur in many (and probably most) cancers. Weakness implies generalized physical debility and lethargy refers to the inability to maintain normal physical and mental effort. The intensity of the components of failure to thrive is not necessarily related to tumor size, tissue origin, cell type, or degree of differentiation. Pharmacologic therapy can promote nutrition by increasing appetite, controlling nausea and vomiting, improving gastric reflux, and sometimes by relieving obstruction. Clear-cut improvement in anorexia has been documented with progestational drugs, especially megestrol acetate. At 800 mg/d, patients showed improved appetite, nonfluid weight gain, and reduction in nausea and vomiting. In a trial of chemotherapy with and without megestrol in patients with extensive small cell lung cancer, 42 however, neither quality of life nor survival time was improved with megestrol. Corticosteroids are less expensive than progestational agents but also have more significant side effects. These maneuvers include mouth care, maintenance of regular bowel movements, and stressing patient choice in food preparation. Family and friends eating with the patient creates a shared experience that may be beneficial to all. On occasion, oral comfort entails more intensive therapy to treat mucositis due to antitumor therapy or oral thrush.
Whenever possible monotherapy using the lowest effective therapeutic dose should be employed medications hyperthyroidism purchase praziquantel with visa. Maternal disorders Several maternal disorders have been identified in which the risk of fetal malformations is increased medications that cause tinnitus buy praziquantel cheap, including diabetes and phenylketonuria medicine 832 purchase praziquantel 600mg fast delivery. The risk of congenital malformations in the pregnancies of diabetic women is two to three times higher than that in the general population but may be lowered by good diabetic control before conception and during the early part of pregnancy medications given during labor generic praziquantel 600mg with visa. In phenylketonuria the children of an affected woman will be healthy heterozygotes in relation to the abnormal gene, but if the mother is not returned to a carefully controlled diet before pregnancy the high maternal serum concentration of phenylalanine causes microcephaly in the developing fetus. Maternal infection early in gestation may cause structural abnormalities of the central nervous system, resulting in neurological abnormalities, visual impairment and deafness, in addition to other malformations, such as congenital heart disease. When maternal infection occurs in late pregnancy the risk that the infective agent will cross the placenta is higher, and the newborn infant may present with signs of active infection, including hepatitis, thrombocytopenia, haemolytic anaemia and pneumonitis. Rubella embryopathy is well recognised, and the aim of vaccination programmes against rubella-virus during childhood is to reduce the number of non-immune girls reaching childbearing age. The presence of rubella-specific IgM in fetal or neonatal blood samples identifies babies infected in utero. Only 3% of newborn infants, however, have evidence of cytomegalovirus infection, and no more than 5% of these develop subsequent problems. Infection with cytomegalovirus does not always confer natural immunity, and occasionally more than one sibling has been affected by intrauterine infection. Unlike for rubella, vaccines against cytomegalovirus or toxoplasma are not available, and although active maternal toxoplasmosis can be treated with drugs such as pyrimethamine, this carries the risk of teratogenesis. Herpes simplex infection in the newborn infant is generally acquired at the time of birth, but infection early in pregnancy is probably associated with an increased risk of abortion, late fetal death, prematurity and structural abnormalities of the central nervous system. Maternal varicella infection may also affect the fetus, causing abnormalities of the central nervous system and cutaneous scars. The risk of a fetus being affected by varicella infection is not known but is probably less than 10%, with a critical period during the third and fourth months of pregnancy. Techniques for undertaking diagnosis on single cells has more recently made preimplantation diagnosis of some genetic disorders possible. They must be supported during this time and given full explanation of results as soon as possible. Most tertiary centres have developed fetal management teams consisting of obstetricians, midwives, radiologists, neonatologists, paediatric surgeons, clinical geneticists and counsellors, to provide integrated services for couples in whom prenatal tests detect an abnormality. Since an abnormal result on prenatal testing may lead to termination this course of action must be acceptable to the couple. Careful assessment of their attitudes is important, and all couples who elect for termination following an abnormal test result need counselling and psychological support afterwards. Couples who would not contemplate termination may still request a prenatal diagnosis to help them to prepare for the outcome of the pregnancy, and these requests should not be dismissed. A pregnancy may be at increased risk of Down syndrome or other chromosomal abnormality because the couple already have an affected child, because of abnormal results of biochemical screening, or because of advanced maternal age. The actual risk is usually low, but prenatal testing is often appropriate, since this allows most pregnancies to continue with less anxiety. There is a higher risk of a chromosomal abnormality in the fetus when one of the parents is known to carry a familial chromosome translocation or when congenital abnormalities have been identified by prenatal ultrasound scanning. In other families, a high risk of a single gene disorder may have been identified through the birth of an affected relative. Screening for carriers of cystic fibrosis is also possible, but not generally undertaken on a population basis. In many mendelian disorders, particularly autosomal dominant disorders of late onset and X linked recessive disorders, family studies are needed to assess the risk to the pregnancy and to determine the feasibility of prenatal Figure 14. Severity of the disorder Several important factors must be carefully considered before prenatal testing, one of which is the severity of the disorder. For many genetic diseases this is beyond doubt; some disorders lead inevitably to stillbirth or death in infancy or childhood. The decision to terminate an affected pregnancy may be easier to make if there is no chance of the baby having prolonged survival. Equally important, however, are conditions that result in children surviving with severe, multiple, and often progressive, physical and mental handicaps, such as Down syndrome, neural tube defects, muscular dystrophy and many of the multiple congenital malformation syndromes.
The recording from each electrode reflects the electrical activity of the underlying brain region medicine 031 purchase cheap praziquantel. In other phases of sleep and in various wakeful states treatment uti praziquantel 600mg with mastercard, the pattern changes medicine definition purchase cheap praziquantel online, but always in a predictable manner symptoms juvenile diabetes order cheap praziquantel on-line. Recorded from the scalp, the electrical potential exhibits a waveform with time on the x-axis and voltage on the y-axis. When awake, the oscillations occur much faster when the person is relaxed (alpha) or reflect a combination of many components when the person is excited. The components of the waveform are named according to its polarity, N for negative and P for positive, and the time the wave appeared after stimulus onset. Thus, a wave tagged N100 is a negative wave that appeared 100 milliseconds after a stimulus. Care must also be used when looking at the wave polarity, because some researchers plot negative in the upward direction and others in the downward direction. This trait has made them an important tool for clinicians evaluating sensory systems. Waves that occur 100 ms after the stimulus presentation are no longer solely derived from sensory processing, but are modulated by attention. It is found when a stimulus is physically deviant from the preceding stimuli, such as when a G tone is heard after a series of C tones. The P300 wave is seen when an attended stimulus is presented, especially if the stimulus is relatively rare. It differs from the N200 in that the surprise event here might be a violation of semantics. Another approach used by many cognitive neuroscientists focuses on how brain activity is modulated in response to a particular task. By averaging the traces, investigators can extract this signal, which reflects neural activity that is specifically related to the sensory, motor, or cognitive event that evoked it- hence the name event-related potential (Figure 3. For example, the visual evoked potential can be useful in diagnosing multiple sclerosis, a disorder that leads to demyelination. When demyelination occurs in the optic nerve, the electrical signal does not travel as quickly, and the early peaks of the visual evoked response are delayed in their time of appearance. Note that these localization claims are based on indirect methods, because the electrical recordings are actually made on the surface of the scalp. For early components related to the transmission of signals along the sensory pathways, the neural generators are inferred from the findings of other studies that use direct recording techniques as well as considerations of the time required for neural signals to travel. This approach is not possible when researchers look at evoked responses generated by cortical structures. The auditory cortex relays its message to many cortical areas, which all contribute to the measured evoked response, making it much harder to localize these components. For example, as we will see in Chapter 7, evoked responses can tell us when attention affects how a stimulus is processed. The evoked potential shows a series of positive (P) and negative (N) peaks at predictable points in time. In this auditory evoked potential, the early peaks are invariant and have been linked to neural activity in specific brain structures. Later peaks are task dependent, and localization of their source has been a subject of much investigation and debate. The color represents "power," or the activity (as indicated at the bar on the right, where blue is the lowest activity and red is the highest) of a particular frequency at various times both before and after the stimulus is presented. Presumably, recognizing something requires not only that individual neurons fire but also that they fire in a coherent manner. The rhythms are defined by the frequency of the oscillations; thus, alpha refers to frequencies around 10 Hz, or 10 times per second (Figure 3. Thus time-frequency analysis is a way to characterize two-dimensional signals that vary in time. The electrical current associated with synaptic activity produces small magnetic fields that are perpendicular to the current. Unlike electrical signals, magnetic fields are not distorted as they pass through the brain, skull, and scalp.
Located at the posterior pole of the thalamus is the pulvinar nucleus symptoms zinc deficiency purchase praziquantel uk, which is involved in attention and in integrative functions involving multiple cortical areas symptoms kidney cancer cheap praziquantel 600 mg fast delivery. The hypothalamus is the floor of the third ventricle symptoms kidney cancer purchase praziquantel with paypal, and symptoms dehydration generic praziquantel 600 mg with visa, as the name suggests, it sits below the thalamus. Hypothalamus the main link between the nervous system and the endocrine system is the hypothalamus, which is the main site for hormone production and control. The two bumps seen on the ventral surface of the brain, the mammillary bodies, belong to the small collection of nuclei and fiber tracks contained in the hypothalamus (Figure 2. Extending from the hypothalamus are major projections to the prefrontal cortex, amygdala, spinal cord, and pituitary gland. The hypothalamus controls the functions necessary for maintaining the normal state of the body (homeostasis). It sends out signals that drive behavior to alleviate such feelings as thirst, hunger, and fatigue, and it controls body temperature and circadian cycles. It accomplishes much of this work through the endocrine system and via control of the pituitary gland. The hypothalamus produces hormones, as well as factors that regulate hormone production in other parts of the brain. For example, hypothalamic neurons send axonal projections to the median eminence, an area bordering the pituitary gland. There it releases peptides (releasing factors) into the circulatory system of the anterior pituitary gland. These in turn trigger (or inhibit) the release of a variety of hormones from the anterior pituitary into the bloodstream, such as growth hormone, thyroid-stimulating hormone, adrenocorticotropic hormone, and the gonadotropic hormones. Hypothalamic neurons in the anteromedial region, including the supraoptic nucleus and paraventricular nuclei, send axonal projections into the posterior pituitary gland. There they stimulate the gland to release the hormones vasopressin and oxytocin into the blood to regulate water retention in the kidneys, milk production, and uterine contractility, among other functions. Circulating peptide hormones in the bloodstream can also act on distant sites and influence a wide range of behaviors, from the fightor-flight response to maternal bonding. The hypothalamus can itself be stimulated by hormones circulating in the blood that were produced in other regions of the body. The hypothalamus is important for the autonomic nervous system and endocrine system. The pituitary gland releases hormones into the bloodstream where they can circulate to influence other tissues and organs. A Guided Tour of the Brain 47 the Telencephalon: Limbic System, Basal Ganglia, and Cerebral Cortex Toward the front of and evolutionarily newer than the diencephalon, the telencephalon develops into the cerebrum, which includes the cerebral cortex, the limbic system, and the basal ganglia. Compared to the diencephalon, the anatomy (and functions) of the forebrain above the thalamus are less straightforward. Instead of a rather linear stacking of structures, it forms a clump of structures found deep within the cerebral hemispheres nestled over and around the diencephalon. In the 17th century, Thomas Willis observed that the brainstem appeared to sport a cortical border encircling it and named it the cerebri limbus (in Latin, limbus means "border"). For better or for worse, in a move that began to tie the area with specific functioning, Paul Broca in 1878 renamed it the grand lobe limbique and suggested that it was a primary player in olfaction. In the 1930s James Papez (pronounced "payps") first suggested the idea that these structures were organized into a system for emotional behavior, which led to the use of the term Papez circuit. It was named the limbic system by Paul MacLean in 1952 when he suggested the addition of more brain areas, such as the amygdala and prefrontal cortex. Note that the limbic system is neither anatomically nor functionally organized to the degree that other systems are in the brain. In fact, some researchers feel that the limbic system is sufficiently nebulous that the concept should be discarded or reevaluated.
St. Augustine Humane Society | 1665 Old Moultrie Rd. | St. Augustine, FL 32084 PO Box 133, St. Augustine, FL 32085 | Phone (904) 829-2737 |info@staughumane.org
Hours of Operation: Mon. - Fri. 9:00am - 4:00pm Closed for Lunch Each Day: 12:30pm - 1:30pm
Open Sat. by Appointment Only for Grooming General Operations Closed: Sat. and Sun.